Slides and video transcripts for the new NHS Children & Young People’s (CYP) Gender Dysphoria services seen by Trans Safety Network include claims that “safeguarding concerns” facing trans CYP include “coercion from parents and carers” into transition. The materials appear to suggest that clinicians should suspect a role for “fictitious illness” or “secondary gains” in trans youth, casting doubt on their account of their own identity.
One expert Trans Safety Network spoke to about the training materials raised major concerns about the training, stating that the materials had “nothing to offer” happy trans children and young people seeking support to transition and that the materials downplayed the harms of transphobia, made false claims about social transition and cited material by transphobic clinicians.
A clinician involved in delivering the training, Anna Hutchinson, was previously involved in delivering “gender exploratory” training materials to NHS clinicians, which cited a number of pro-conversion therapy organisations and individuals. Gender Exploratory Therapy is regarded by many LGBTQ+ advocates as a euphemism for conversion practices. Hutchinson was a speaker at the controversial CAN-SG “First do no harm” conference, which faced criticism alleging that it was promoting conversion practices.
Hutchinson also spoke at an event at the 2024 Labour Party Conference hosted by the anti-trans organisation Labour Women’s Declaration, which laid out, among other issues, the group’s opposition to a criminal ban on sexual orientation and gender identity conversion practices. Hutchinson used her talk to scaremonger about a proposed conversion practices ban, misrepresented historical and contemporary conversion practices and suggested that a ban would interfere with implementation of the Cass review.
Training materials
Trans Safety Network obtained copies of the slides and transcripts of videos used in the induction training for the new CYP Gender Dysphoria services via a Freedom of Information request. The training was delivered by the Academy of Royal Medical Colleges and commissioned by NHS England. According to the documents received by TSN, there were seven videos consisting of slides and spoken material which clinicians watched remotely. There was also a single face to face training day, which TSN was not given any detail on other than that the training days took place between February and June 2024.
TSN spoke to Cal Horton, an academic researching trans inclusion and vocal critic of cis-supremacist approaches to trans health, about the training. Horton raised a number of concerns, stating that the training “provides a lot of miseducation” and fails to provide professionals with useful information to support trans CYP.
- Lack of clarity on social transition: Social transition refers to any steps taken in transition that are not medical, such as changing one’s name, coming out as trans or changing gendered presentation (clothes, personal grooming). Horton raised concerns with TSN about how the training materials discuss social transition. The materials claim that social transition is poorly defined, which Horton rejects, saying that “has a clearly accepted definition both in the academic literature, in clinical practice and in everyday usage.” According to Horton the training materials “misrepresent existing literature, which find zero harms and many, many benefits of social transition” with “No mention of the harms of denying social transition, no mention of the numerous studies showing very significant benefits.” Additionally, we at TSN would question the extent to which social transition is properly the business of clinicians, rather than a form of free expression that trans people undertake in order to live our lives in a way that makes most sense for us.
- Poor recognition of harms of transphobia: While the training does briefly mention that transphobia can do harm in a few places, it makes some notable omissions. Horton highlighted to us that the training frequently seems to gloss over the harms of transphobia, for example in a session on safeguarding (session 7), the training briefly mentions transphobia but in terms of direct harm from families only directly mentions “criticism, hostility or other physical or emotional abuse related to same-sex attraction or gender expression,” without mentioning rejection or abuse specifically for being trans, despite this being a significant cause of harm to trans CYP.
- Inappropriate choices of literature: According to Horton, the training materials make some concerning choices with respect to drawing on existing research. In particular Horton points out that the training session that discusses models of care (session 2) “omit[s] all the most important texts that a new clinician in this area should read” and cites the work of highly controversial clinicians. TSN note that the materials cite Canadian sexologist Kenneth Zucker, who has been the subject of credible allegations of gender identity conversion practices leading to the clinic he worked at being shut down.
Overall, Horton said that they did not think the training materials provided adequate information on how to support trans CYP.
“[F]rom the materials it is very clear that they have literally nothing to offer a happy trans kid, or a kid whose only problem is related to transphobia/cisnormativity/gender minority stress/dysphoria” - Dr Cal Horton
At various points, the training calls for a “biopsychosocial” approach, with the first video session calling for clinicians to “Ensure that all patients are offered a comprehensive biopsychosocial assessment.” In the final video, on safeguarding concerns, the training material appears to suggest both that trans CYP’s parents may be pressuring them into transition or that trans identity may be linked to “fictitious or fabricated illness” or driven by “secondary gains.”
“Coercion from parents and carer or the potential for secondary gains that can shape a child's gender understanding and expression. Parents or carers may have become heavily invested in one outcome and can drive a child’s social or medical transition.” - AoMRC, CYP gender service training materials
“Perplexing presentations such as functional disorders or fictitious or fabricated illness. These are amongst the most challenging clinical presentations that can occur alongside presentations for professional support with gender incongruence.” - AoMRC, CYP gender service training materials
The biopsychosocial approach refers to the biopsychosocial model, which is a model for understanding disability, illness and health. There are multiple biopsychosocial models of healthcare, some of which are closely associated with medical gatekeeping and claims of fictitious illness and malingering, as discussed in previous TSN reporting.
In theory, the biopsychosocial model incorporates biological, social and psychological domains to offer a more holistic approach to healthcare, including psychiatric care. Its origins in psychosomatic medicine affect its application across the board with the model frequently ignoring some of the domains to the preference of others. In practice, it usually relies more heavily on psychological factors which in the case of the original version were primarily psychoanalytic. The version in use today relies more on a cognitive behavioural approach.
The biopsychosocial model was proposed as a means of moving away from mind/body dualism. Moving away from mind/body dualism is not a bad thing. However the biopsychosocial model fails to do this coherently. This has left patients with medically unexplained symptoms who fall in the “mind-body borderlines” of psychosomatic medicine (where the original model came from) subject to treatments and practices that are afforded less scientific scrutiny than elsewhere in the medical system. It is unclear how a biopsychosocial approach to trans healthcare is envisaged in this training, especially given that there is no singular biopsychosocial model.
Existing literature on the biopsychosocial model pertaining to trans people covers a wide range of disciplines and potential health factors. This ranges from factors for physiotherapists to consider, to advice for anesthesiologists who may be dealing with trans patients to literature by and for gender service clinicians. Some of the literature in the gender clinician category is harmful and some not, with the latter study linked to having been criticised by AusPATH as having a “clear agenda” against affirmation of trans CYP and allegedly misrepresenting its data to inflate youth detransition rates. The biopsychosocial model has also been cited by transphobic Catholic bishops and used in guidance for schools in Australia calling for teachers not to affirm trans students and describing being trans as a “psychological condition” for the majority of trans children. The emphasis on secondary gains elsewhere in the training materials suggests this more harmful biopsychosocial approach, and an implied link to functional and psychosomatic disorders, or that being trans is a form of this, mirroring disablist research discussed in our previous reporting.
“Secondary gain” has multiple meanings and it can be difficult to know what is inferred without further context. In the context of functional disorders, it is likely to be in the original Freudian context of unconscious motivations although some literature on functional disorders does define “secondary gains” as conscious and deliberate and links them to fictitious and fabricated disorders (for attention) and malingering (for financial gain or exemptions). Although others describe the same motivators as unconscious as discussed here. In the context of trans CYP and their parents allegedly pushing them towards transition it is likely to both depending on the professional’s assessment.
Fictitious or fabricated illness was previously known as Munchausen's syndrome. Fabricated or induced illness in another was previously called Munchausen Syndrome by proxy and is a serious form of child abuse. Safeguarding in educational and medical settings is crucially important particularly where a child has an existing disability as research estimates suggest that disabled CYP are three times more likely to face abuse or neglect.
However, abuse involving fictitious or fabricated illness is thought to be extremely rare but accusations of it are not. Parents of disabled CYP are at particular risk of false allegations, particularly if the parent or carer is disabled themselves or makes a complaint about their treatment. According to a 2023 research report by the University of Leeds and the children's brain condition charity, Cerebra, NHS practitioners were the source of most allegations, followed by schools and then local authority children's services. The report also found that most (84%) resulted in no follow-up action and that disabled parents were more likely to face allegations as were parents with other “protected characteristics.” The report found that 50% of allegations arose following a complaint against a relevant public body and that unsubstantiated allegations were traumatic for the entire family. The report called for a review of the 2021 RCGP guidance on Perplexing Presentations (PP) /Fabricated or Induced Illness (FII) in Children and stated that its “alerting signs” on which the guidance suggests reports should be made, are not based on evidence and “unsupported by any peer-reviewed research.”
Trans CYP are more likely to be autistic and autistic people are more likely to have chronic health conditions, many of which are often inappropriately included in the “functional” or “psychosomatic” umbrella such as Myalgic Encephalomyelitis and Fibromyalgia. Autistic people are also more likely to have a condition in the considered rare class of connective tissue disorders including Ehlers-Danlos Syndrome (EDS). EDS, particularly the hypermobile type, is difficult to diagnose and parents/carers are frequently accused of fabrication and/or abuse due to injuries caused by the condition in undiagnosed children.
Therefore trans CYP are far more likely to be disabled CYP with “perplexing presentations”. We are concerned that supportive parents/carers, particularly should they complain about their children’s treatment regarding their gender from NHS or Education services are at serious risk of being accused of fabricating their child’s trans identity for “secondary gain”. This concern is amplified for trans CYP who are either disabled themselves or have a disabled parent/carer.
The suggestions of a link to fictitious illness and secondary gains in the training pathologise trans and gender diverse youth and prime clinicians to treat trans and gender diverse CYP's identifies with suspicion and skepticism. The suggestion that trans CYP are more likely to present with fictitious illness additionally poses a risk of disabled trans CYP not being believed when reporting symptoms of illness.
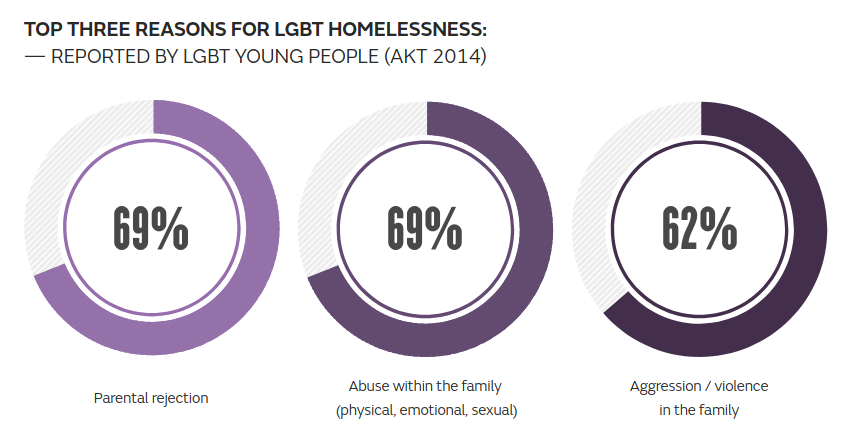
While a small number of documented cases of parental coercion in relation to transition do exist, this is an extremely rare phenomenon in comparison to harms from parental transphobia, with some research suggesting that a majority (56%) of conversion practices are carried out by family. Research by the LGBTQ+ housing charity AKT has found that LGBTQ+ young people are disproportionately represented among homeless and precariously housed youth, frequently related to rejection or hostility from family. Almost two thirds of LGBTQ+ youth with experience of homelessness responding to a 2021 survey by the charity reporting that they “felt frightened or threatened by their family members before they became homeless.” The training has relatively little to say on specifically transphobic hostility from family members and nowhere is risk of homelessness, a major safeguarding issue for trans CYP, discussed in the training.
Four out of the seven video sessions contained mentions of “gender-related distress.” This term, whose origins in conversion therapy were explored in Ilya Maude’s recent piece for Trans Safety Network, is used within the training to suggest that clinicians should, in some cases, seek to “locate the issue” of a young person’s gender dysphoria in external factors. As outlined in Maude’s reporting for TSN, such rhetoric can easily serve as justification for a “love the sinner, hate the sin” approach to gender identity conversion practices. The focus on reframing the language by which CYP describe their experiences would fit within the CBT based modes of conversion practices discussed by Maude. We asked NHS England, the AoMRC and Hutchinson whether this is consistent with conversion practices, none provided any comment on this issue.
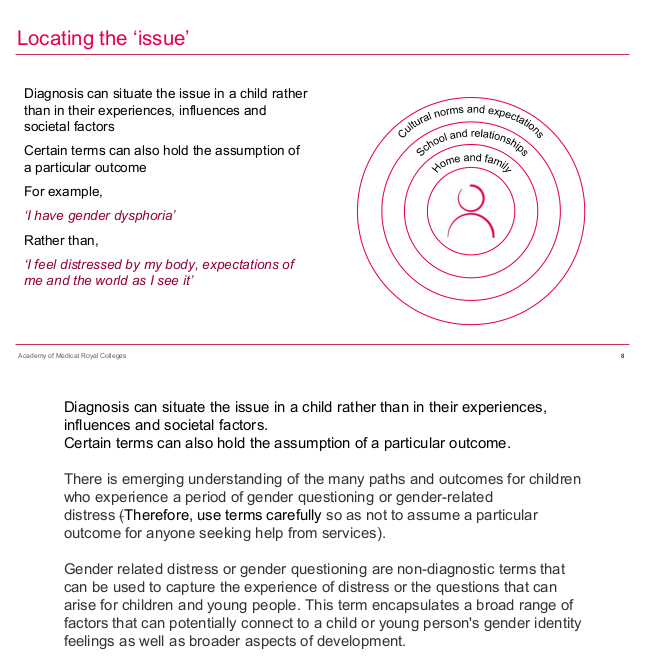
“Gender-related distress” is a term relatively new to the training literature but features prominently within it. It also features heavily within the Cass Review and before that in the article by Canvin et al. (2022) in the language of third-wave cognitive behavioural therapy as further discussed by Ilya Maude. The appearance of this terminology appears to be a misappropriation of language from the disabled people and psychiatric service user movements by alluding to the term “mental distress”. Some parts of these movements began using the term “mental distress” to refer to symptoms of psychiatric impairments exacerbated by social factors to reframe their experiences and shift the focus back onto the maddening aspects of society, rather than individual pathology. As a result of that activism, this term is now commonplace within the language of mental health charities and some psychiatric nursing literature. This is sometimes used genuinely but often against the intentions of the usage by the survivor movement - still blaming the individual for social issues via a lack of “distress tolerance”. This use within gender service literature looks like an attempt to minimise the need to treat gender dysphoria by constructing a mental illness that presents like gender dysphoria but isn’t gender dysphoria. Calling this construct “gender-related distress” is a misleading use of language that will be familiar to healthcare professionals and gives harmful practices the appearance of progressiveness.
“Gender-related distress” also features prominently in training materials produced by Explore Consultation, a clear throughline can be seen from this to this newer induction training produced with involvement of Explore Consultation members. While the newer training avoids directly mentioning organisations like Bayswater Support Group and Genspect, the previous training by Explore was far less cautious. Explore’s training materials, which list Hutchinson as an author, favourably cite:
- Bayswater Support Group, a conversion practices advocacy organisation recently exposed by a TBIJ investigation as engaging in a number of harmful practices, including isolating trans CYP from their friends, destroying their belongings and blocking children from accessing services such as Childline, mental healthcare and rape crisis services in order to prevent them from contacting services that may affirm their identity.
- Genspect, an umbrella organisation of pro-conversion practices groups whose director has stated that she aims to prevent CYP from being trans. Genspect supports a group who have called for the NHS to “target 100% desistence” (essentially an explicit call for gender identity conversion practices for all trans people) and a blog site by anti-trans parents that has claimed that the popular video game MInecraft can cause children to become trans. Genspect have been described as an “anti-LGBTQ hate group” and one of the “key hubs of anti-LGBTQ+ pseudoscience” by the Southern Poverty Law Centre.
Labour Women’s Declaration
Content warning: The following section includes discussion of conversion practices, including physical and sexual abuse of children and young people. Some sources linked to describe abuse in explicit detail.
At the recent 2024 Labour Party conference, LWD held a meeting within the conference where Hutchinson appeared as a speaker and one Labour MP in attendance argued against a ban on conversion practices.
Labour Women’s Declaration (LWD) are a gender critical organisation operating within the Labour Party that seeks to push party policy in an anti-trans direction. LWD are listed as a “supporting organisation” of the extreme, eliminationist, transphobic organisation Women’s Declaration International (WDI, previously known as WHRC) and have signed their “Women’s declaration”, a document that calls for banning trans women from all women’s spaces and for the defunding of medical research into trans women’s fertility. WDI have previously called for “transgenderism” to be “eliminated” in a bizarre submission to a parliamentary consultation that claimed that niche pornography is responsible for trans women’s gender identity and have previously been involved in spreading misinformation suggesting that major LGBTQ+ organisations seek to legalise child sexual abuse.
LWD have publicly attacked the female Olympic boxers Imane Khelif and Lin Yu-Ting, who have been the targets of an interphobic harassment campaign started by anti-trans far right website Reduxx. LWD shared quotes from an article that falsely describe the two women as “biological males punching a bunch of women in the face.” Speaking on a criminal complaint lodged by Khelif regarding the harassment she has experienced, her lawyer described the campaign against her as “misogynist, racist and sexist.”

LWD have made a public statement in support of failed Labour council candidate Laura Pascal after she was briefly suspended as a candidate by the party after complaints about transphobic comments she had made, shared and boosted on social media, including one comparing trans influencer Dylan Mulvaney’s day to day existence to blackface.
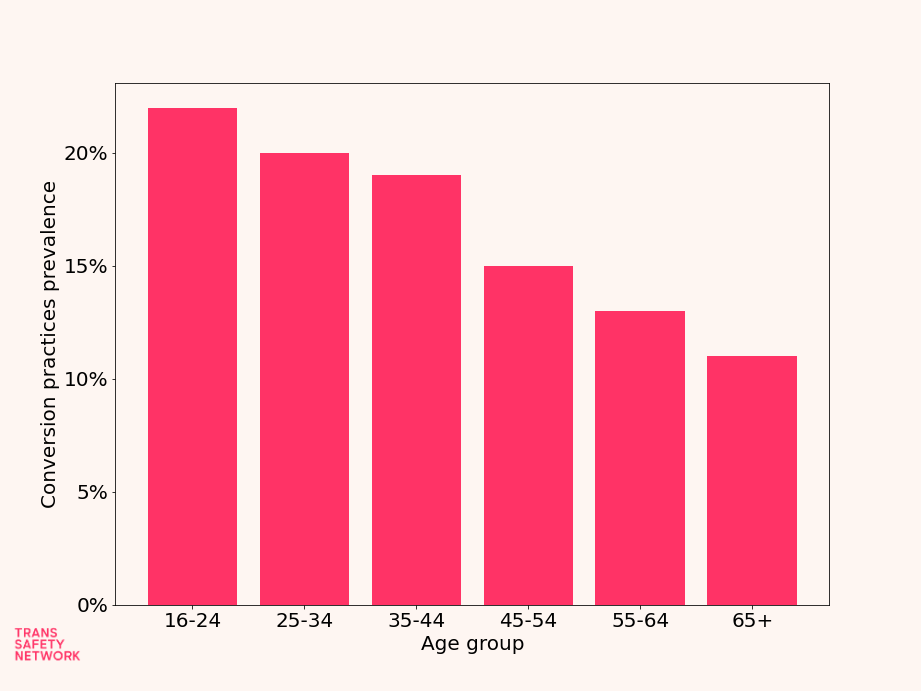
LWD’s website includes a briefing on conversion therapy that claims that there is “no contemporary evidence that [conversion practices] are taking place in the UK,” despite research by Galop showing that 1 in 5 LGBTQ+ people responding to their survey had been subjected to conversion practices, with younger age groups more likely to have experienced such practices, indicating what Galop describe as a “current and ongoing” issue.
It is troubling in the extreme that Hutchinson, a clinician directly involved in providing training to other clinicians working with trans CYP, would speak at an event by an organisation with a clear anti-trans bias that seeks to deny and minimise real and ongoing abuse of vulnerable trans and gender diverse people.
During her talk at the meeting, where she was explicitly named as involved in delivering training for NHS CYP gender services, Hutchinson claimed that conversion therapy was largely a thing of the past and had historically been done specifically to “same sex attracted adults,” suggesting that it is inappropriate to use the same terminology to discuss the treatment of “gender questioning children.” Hutchinson further suggests that it is inappropriate to refer to contemporary conversion practices as such, using the extreme harms of aversion therapy (the practice of torturing patients with electric shocks or emetic drugs to alter behaviour) as a baseline and implicitly denying that other conversion practices should be named as such. These claims minimise contemporary conversion practices. Evidence gathered by Galop demonstrates that conversion practices are an ongoing issue that can include serious violence and in some cases sexual violence (also known as corrective rape). The International Rehabilitation Council for Torture Victims’ Independent Forensic Experts Group has previously stated that “All forms of conversion therapy, including talk or psychotherapy, can cause intense psychological pain and suffering.”
As to Hutchinson’s claims that only “same sex attracted adults” were subjected to aversion therapy, there is a wealth of historical evidence that trans people were among those subjected to "aversion therapy" by the NHS and that LGBTQ+ CYP were subjected to serious, violent conversion practices in the period discussed, with one paper identifying cases of LGB children as young as 13 experiencing conversion practices (including one case of sexual abuse of a 14 year old) and BBC reporting detailing the case of a trans woman who first underwent aversion therapy at the age of 17. There are also many accounts of young adults being subjected to aversion therapy, including the account of one gay man who was forced to undergo the process under threat of expulsion from school at the age of 18.
In TSN’s opinion, this denial of the seriousness of today’s conversion practices and dismissal of the experiences of some survivors of aversion therapy on the basis of their age or gender identity is disturbing from a clinician working with trans CYP.
In the meeting Hutchinson would go on to suggest that “malicious accusations” of conversion therapy are commonplace and a serious problem, suggesting that this is a reason for extreme caution and scrutiny of any state measures aiming to end the practice. This is incongruous with the reality that existing rules by regulatory bodies barring conversion practices appear to be largely unenforced, with the GMC unable to even provide reliable numbers on how many complaints it receives in this area. Hutchinson stops short of openly opposing a ban on conversion therapy in her talk, but repeatedly calls for clinicians to be “protected” from possible accountability for their treatment of LGBTQ+ patients and scaremongers about the possibility that a ban on conversion practices would make the implementation of the Cass review more difficult.
TSN are deeply concerned about what Hutchinson, a clinician working with trans children and young people and involved in the training of other clinicians, considers an appropriate implementation of the Cass review to be if this would be potentially hampered by a ban on conversion practices. Hutchinson said in a statement to TSN that Cass herself has “concerns about the conversion practices bill,” citing a Guardian article quoting Cass.
TSN reached out to NHS England, the Academy of Medical Royal Colleges and Anna Hutchinson for comment. NHS England declined to comment, referring us to the AoMRC as the providers of the training. The AoMRC declined to comment on questions about conversion practices, Hutchinson’s conduct or the risks of homelessness and abuse for trans CYP, but stated that the training materials were “produced wholly in accordance with the findings of the Cass Review.” The AoMRC employee TSN contacted referred to a statement by the AoMRC calling for clinicians not to question "the validity of the evidence and consequently the findings" of the Cass review because this would risk "greater polarisation.” We asked the AoMRC whether this is consistent with the principles of serious scientific inquiry and evidence based medicine, at time of writing we have not received a response. Anna Hutchinson said in a statement that she supports evidence based medicine and that all of her work is “in line with the recommendations of The Cass Review.” Hutchinson did not provide any comment on the inaccuracies about historical and contemporary conversion practices in her talk, her association with an anti-trans organisation or the specific issues of abuse of trans CYP by family members.