Trans Safety Network are extremely concerned about documents we have acquired which show that South London and Maudsley NHS Mental Health Trust hired a consultancy called Explore Consultation to provide training on a “Gender Exploratory Approach” to Child and Adolescent Psychiatrists. Training materials we acquired promoted links to and material from multiple conversion therapy lobby groups including Genspect. The training was addressed to the Lambeth CAMHS team.
We urge the NHS to take these concerns seriously and develop safeguarding against further incursions by Genspect associates into CAMHS gender services, especially in light of previous revelations that they were heavily involved in another training conference which had to be cancelled for safeguarding reasons.
Who are Explore Consultation?
The consultancy, Explore Consultation, is (according to a flyer acquired by Trans Safety Network) is composed of
- Dr Anna Hutchinson
- Dr Tilly Langton
- Anastassis Spiliadis
- Dr Anna Churcher Clarke
- Dr Natasha Prescott
Investigation of the consultancy itself revealed that it has no publicly visible presence to speak of. The domain name for the email on the flyer was registered last year, on 17th March 2021. We were unable to identify a companies house registration in that name.
{kind=link}
Of these five members, two have been noted in an Anti-Trans Conversion Therapy Map of Influence published by United States based anti-conversion therapy organisation Health Liberation Now, owing to their professional associations and proximity with figures in conversion therapy advocacy. Spiliadis and Hutchinson are noted in the map in particular for their links to Genspect (and involvement in spuriously separate front organisations like ICGDR which have an almost complete overlap with Genspect’s public membership).
Genspect campaign for bans on trans affirming therapy around the world, and supports organisations which have called for the NHS to target a 100% desistance rate among trans children (a clear call to conversion therapy), as well as promoted therapists who recommend subjecting trans children to acupuncture and other humiliating rituals to scare them off of the prospect of hormone replacement therapy or surgical scars if they transition. Genspect’s founder Stella O’Malley has described trans minors as being driven by “porn-induced” fantasies about whom she has said others should not have any empathy or sympathy and said that her mission is “more than anything to make sure that children are stopped from medical transition”.
Tilly Langton (also known as Trilby Langton) was hired by The Cass review in November 2021 to conduct research on young people with gender dysphoria. Langton's name is in the author field of the metadata for the slide deck.
What is Gender Exploratory Therapy?
Gender Exploratory Therapy (GET) is a controversial new brand of therapy attempting to market itself as a third way triangulating between the Gender Affirmative Model on the one hand, and “Reparative Model” (the latter is widely elsewhere known as conversion therapy). For example, see the diagram on p.7 of Spiliadis original paper Towards a Gender Exploratory Model, indicating an integration of “acknowledging distress” (on the conceptually “affirmative” side) with working towards “diverse outcomes” (on the conceptually “reparative” side of the diagram).
GET has been criticised in the academic sphere for the ways that while it attempts to play “both sides”, it replicates narratives drawn from Reparative and Reintegrative approaches to Sexual Orientation Conversion Efforts (SOCE). In a review of available academic writing on GET Interrogating Gender-Exploratory Therapy conversion therapy expert Florence Ashley says:
The conceptual fulcrum of the gender-exploratory approach lies in gender exploration through talk therapy, with the goal of identifying why youths have gender dysphoria and/or believe themselves to be trans. Gender dysphoria and self-identification as trans are approached with suspicion and associated by proponents of the approach with unprocessed trauma, childhood abuse, internalized homophobia or misogyny, co-occurring mental illness, social contagion, autism, sexual fetishism, and unconscious drives…
It should be also noted that other than recommending that exploration of what gender dysphoria and identity mean for a given patient is important, it has not until now been clear what else Gender Exploratory Therapy entails, or at which bar it is considered time to accept the trans patient is correct in understanding their identity and needs to transition. This matters because, as Ashley notes:
From a patient-centered standpoint, it is crucial to realize that most individuals who enter a clinical relationship because they are trans or experience gender dysphoria do so for the express purpose of securing access to gender-affirming care and, accordingly, living out their felt gender in everyday life.
This sense of respecting and engaging with the purpose with which most patients engage with gender dysphoria related healthcare is one which is completely absent from prior literature on GET.
The Training contents, day 1
We managed to talk to an individual who attended the training. They told us
“It was definitely framed as “unbiased” regarding “two sides”, which seemed like a red flag, rather than focused on the patient…
…The way that some of them spoke one of them in particular kept bringing up “two sides” when talking about signposting places, she mentioned mermaids and another trans affirmative place, and then pointed out 3 other places… One of them was transgender trend.
From a copy of the slide deck we acquired, the training does exactly that. It tries to “balance” the views of mainstream but non-medical charities like Mermaids and Gendered Intelligence who provide support groups for parents and for children and ways to connect with peers and help development outside of a clinical setting, against organisations which are known for their history of legitimising and even promoting conversion therapy.
Excerpt from slide deck: “Explore learning and consultation. Working therapeutically with young people who experience gender-related distress. Dr Anna Hutchinson, Anastassis Spiliadis, Dr Tilly Langton
The fact that all 3 of these individuals work with children and are willing to have their names on a training document which promotes conversion therapy advocacy groups as part of their professional practice is deeply worrying with regards to the safeguarding implications for the children they work with, and those who will be cared for by the CAMHS professionals they are training.
In fact it is striking to note that a huge amount of effort has been made by “Explore Learning and Consultation” to fixate on politicising the context around trans and gender diverse patients, rather than centring the patient themselves. An early slide (shown below) mixes placards from “Trans Rights” demonstrations, with “Gender Critical”, the logo of the Bayswater Support Group conversion therapy organisation, TikTok, and, bizarrely, placards against austerity. There’s no real attempt here to point out that the conversion therapy organisation mentioned is a risk to children (and our source who attended the training reported no such issues being flagged up as a risk).
![Image of concentric circles. in the centre is “A changing group of young people with varied needs”, with the circle around containing speech bubbles such as “A diversity of outcomes and pathways”, “high rates of co-occurring ASC [Austistic Spectrum Conditions]”, “An underrepresentation of young people of colour”, “The emerging voice of young adults who have detransitioned”.](https://transsafety.network/posts/gender-exploratory-nhs-training/Untitled%202.png)
Image of concentric circles. in the centre is “A changing group of young people with varied needs”, with the circle around containing speech bubbles such as “A diversity of outcomes and pathways”, “high rates of co-occurring ASC [Austistic Spectrum Conditions]”, “An underrepresentation of young people of colour”, “The emerging voice of young adults who have detransitioned”.
The effect of this image overloads the viewer with potentially alarming jargon. While many issues are raised, there is no suggestion here that this constellation is actually explained in a way that allows the trainees to usefully navigate the issues. Trans Safety Network feel that this is a deliberate attempt to muddy rather than clarify the waters at the start of this training. In particular, questions raised such as the changing patient cohort (which is raised many times during the training) will just not be resolved until the Cass Review has run its course and undertaken necessary investigations in order to direct clinicians towards necessary changes in practice.
This “balance”/”two sides” model gets even more ridiculous at a point where they present a slide on transition regret, featuring a video by a trans man who had at the time of this training already followed up with further videos to clarify that he was comfortable in his transition and not detransitioning.
The training warns of “Significant and important policy and legal developments that are changing the landscape of clinical care” citing a legal rulling (Bell v Tavistock, 2020) which was overturned last year, after the original ruling was described as being based on partisan evidence.
![Significant and Important policy and legal developments that are changing the landscape of clinical care. An independent review of child and adolescent services is now underway - Cass Interim report recommends development of more regional centres. [link] Several other European countries also initiating similar reviews — Finland, Sweden and Germany. Recently published NICE review on the evidence for use of puberty blockers, and cross sex hormones. Judicial Review and ongoing hearing and appeals in relation to puberty blocker consent and a wider discussion about the narratives of detransitioners](https://transsafety.network/posts/gender-exploratory-nhs-training/Untitled%203.png)
Significant and Important policy and legal developments that are changing the landscape of clinical care. An independent review of child and adolescent services is now underway - Cass' Interim Report recommends development of more regional centres. [link] Several other European countries also initiating similar reviews — Finland, Sweden and Germany. Recently published NICE review on the evidence for use of puberty blockers, and cross sex hormones. Judicial Review and ongoing hearing and appeals in relation to puberty blocker consent and a wider discussion about the narratives of detransitioners
However, while the overturned Bell 2020 ruling cited above effectively banned puberty blocker consent for under 16s, this was reversed after the appeal court heard that the initial ruling was based on partisan evidence. In effect this training was directly misinforming CAMHS practitioners that the legal environment is far more hostile to transition related medical care than it actually is. This cherry picking and stacking of the evidence base used is a persistent theme.
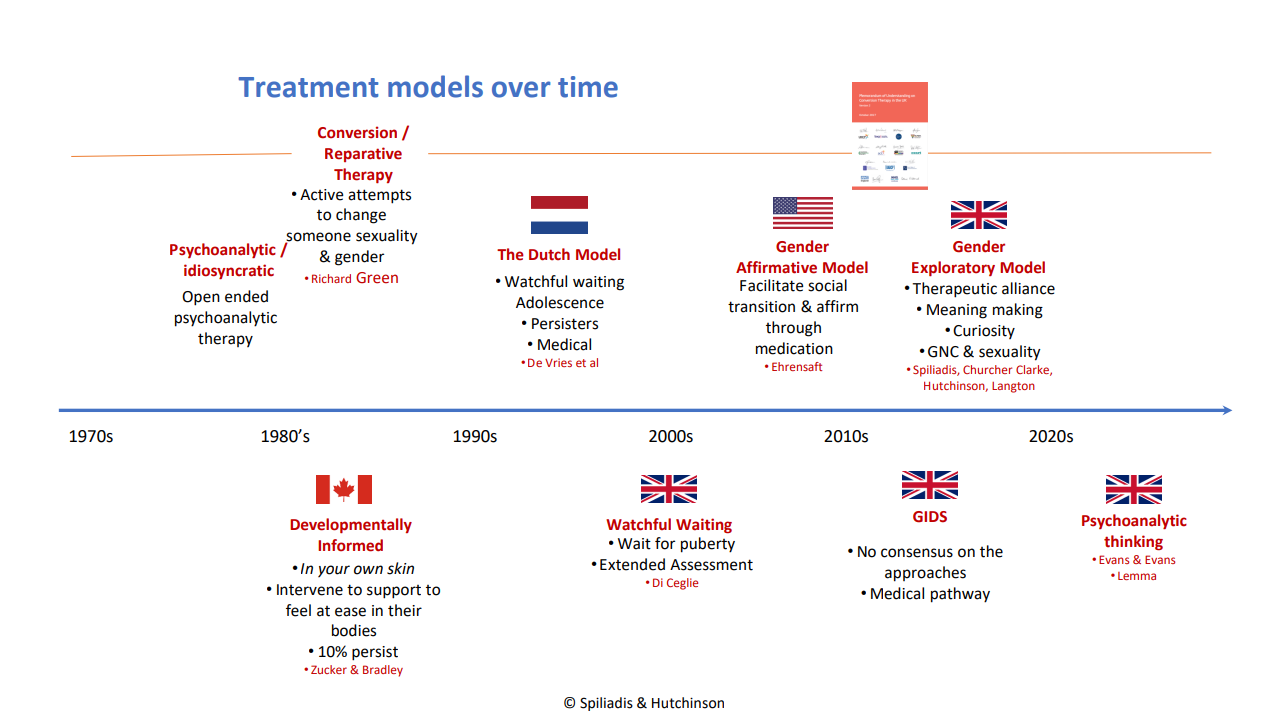
Later on in the training they provide a timeline which conveniently for those marketing “Gender Exploratory” approaches places Gender Exploratory and Psychoanalytic Thinking at the forefront of transgender treatment models. It should be noted that the psychoanalytic approaches to curing Gender Dysphoria have been attempted and rejected as ineffective since, at least, 1954, and has absolutely no evidence base with respect to its efficacy. Conversely the Gender Exploratory Model is a novel theoretical framework which has already raised considerable criticism for its similarity to conversion therapy. Evans & Evans’ book “Gender Dysphoria” has received powerful critiques from the world of academic psychoanalysis,
In one academic review of the Evanses’ book, On trying to pass off Transphobia as Psychoanalysis and Cruelty as “Clinical Logic”, published in The Psychoanalytic Quarterly, Avgi Saketopoulou says
… Despite touting an “objective scientific appraisal” (p. xix), and stating that the authors are “neither ‘pro’ nor ‘anti’ transition” (p. 7) and will “keep an open mind” (p. 8), this highly political volume gives us, instead, a remarkably stale and dangerous recycling of anti-trans rhetoric.
Marcus and Susan Evans are advisory team members of conversion therapy advocacy organisation Genspect, something which this training does nothing to draw attention to. They were also recently subject to strong condemnation on the basis of accusations of promoting conversion therapy by the Polish Sexological Society on a tour visiting the country to promote their theories.
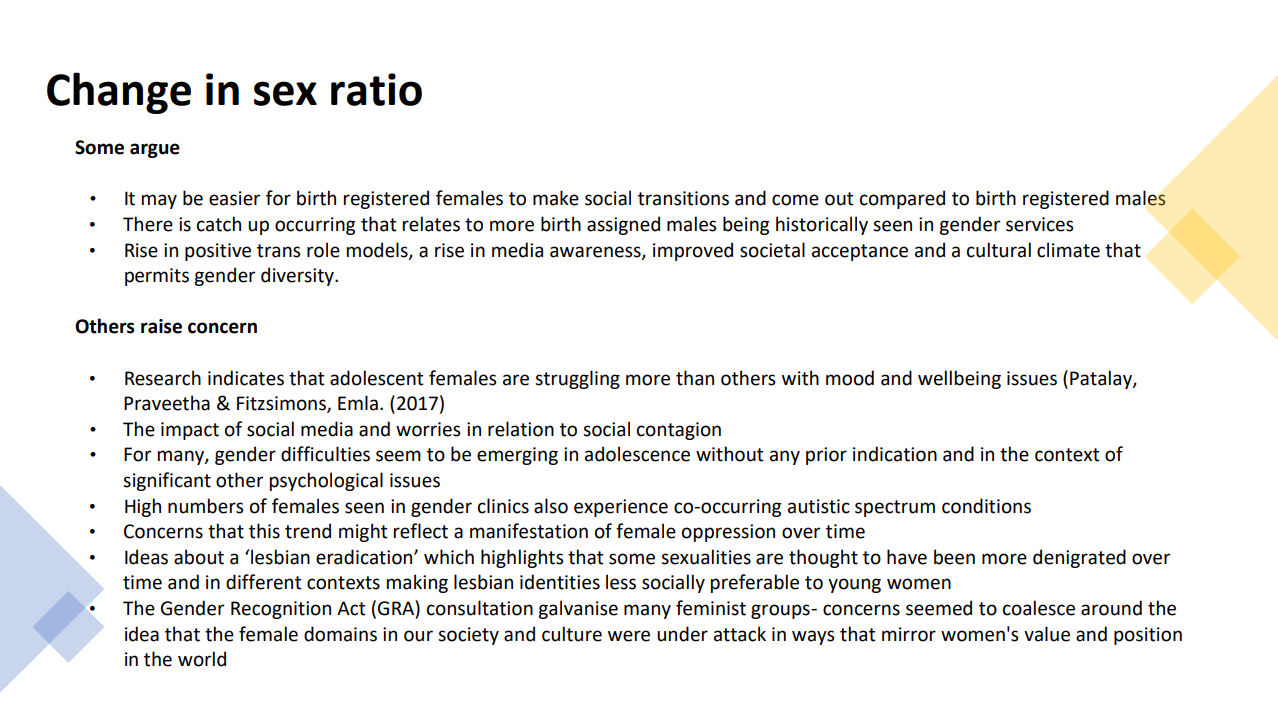
This “both sides, but against affirmation” approach continues throughout the training, with relative figures given for the increase in patients at GIDS (with the starting point being measured from the point at which GIDS started providing the service, and thus relative increase being a meaningless figure), and then debating the changing patient sex ratio in terms of “lesbian eradication” theories. This is despite rising year on year percentages of young people also identifying as gay or lesbian which goes unmentioned. The training continues scaremongering about the risks of trans healthcare somehow being a threat to the values of supporting young LGB people.
They then enter into discussion on the important and delicate subject of desistance and detransition. Their key resource on this is a video from an event run by Genspect which was promoted (with Genspect’s blessing) by Michael K Laidlaw. Laidlaw is involved in the Christian extremist pro-conversion therapy charity IFTCC. Laidlaw himself is also a member of the SPLC designated hate group ACPeds.
The end of Day 1 of the training culminates in the conclusion:
This all highlights the value of providing exploratory approaches that support an ‘opening up and a slowing down’
While Trans Safety Network have nothing against careful exploration in principle and there is inevitably a necessary period of evaluation to assess young people’s capacity to give informed consent for any procedure, we also have to draw attention to the lengthy timelines that on which young trans people in the UK are already receiving treatment. While the vast majority of young people accessing Gender Dysphoria related care sit on waiting lists for years, those who go through the treatment process are already subject to lengthy assessment processes, with phase based introduction of increasingly significant medical interventions as the young person develops. There are doubtless ways in which evidence and guidance around these protocols could be improved (which is by and large the purpose of The Cass Review, still underway).
This call to open up and slow down is a direction to introduce further delays to accessing treatment beyond the existing diagnostic procedures (however these will develop as further evidence emerges).
Day 2
This theme of holding trans people’s awareness of our own gender identities in skepticism continues on the second day, where the slides promote the importance of the “developmental frame” (associated in previous slides with Zucker and Bradley’s efforts to actively deter trans children from persisting in their gender identity) while training raising concerns that (emphasis ours)
Young people who experience high levels of distress need support to make sense of this and interventions that attend to distress without narrowing developmental opportunities or confirming an outcome
The purpose of Gender Exploratory Therapy isn’t just to be neutrally taking a different route to the Gender Affirmative Therapy, it actively dictates that the therapist does not at any point accept the patient’s understanding of themself, or their expectations they may have future transition. The reference to avoiding “narrowing developmental opportunities” frames any efforts that a young trans person may undertake to explore their gender identity through actually transitioning implicitly negatively as “narrowing developmental opportunities”, rather than understanding the possibility that support in practical social transition (for instance) is experienced by many trans people as opening opportunities.
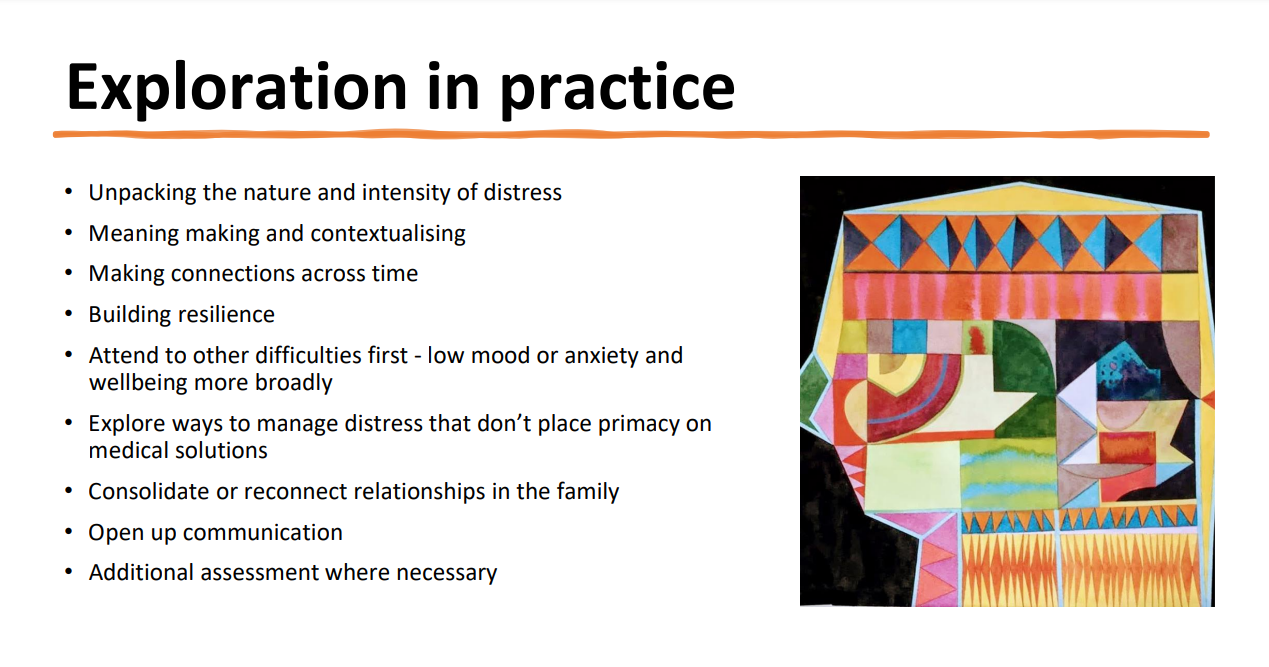
They go on to recommend “building resilience”, “attend to other difficulties first - low mood or anxiety and wellbeing more broadly” and to “explore ways to manage distress that don’t place primacy on medical solutions”. This completely ignores longstanding understandings and guidance, reaffirmed in the latest standards of care by the World Professional Association for Trans Health (and covered extensively in previous editions) that
Indeed, some mental health conditions, such as anxiety (Bouman et al., 2017), depression (Heylens, Elaut et al., 2014; Witcomb et al., 2018), and self-harm (Arcelus et al., 2016; Claes et al., 2015) are more prevalent in TGD people who have not accessed [Gender Affirming Medical and/or Social Treatments].
Gender transition medicine is provided because gender dysphoria is a known cause of low mood and anxiety in some trans people. Putting a priority on avoiding providing this sort of care even in the knowledge that for some patients this will be the most appropriate treatment is decentring the needs of the patient in favour of ideological resistance to it.
Later on they move forward to discussing the issue of non-medical ways that trans youth can address dysphoria, specifically “Social Role Transition” - where a young person adopts any or all of a change of appearance, dress, name, or pronouns.
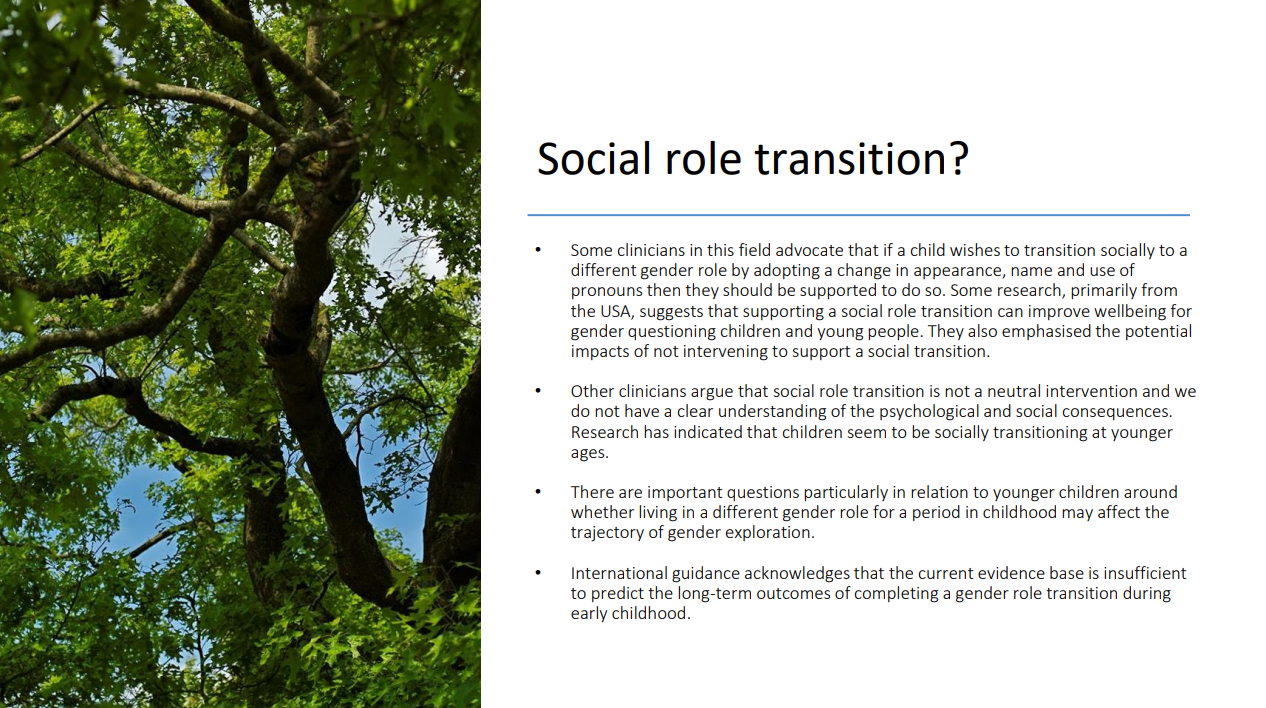
Alarmingly this pair of slides raises “important questions, particularly in relation to younger children, around whether living in a different gender role for a period of childhood may affect the trajectory of gender exploration.” This clearly indicates a belief that decisions around support for young people should be predicated on whether it might help prevent them growing up to be trans, in an echo of the previous work cited by Zucker.
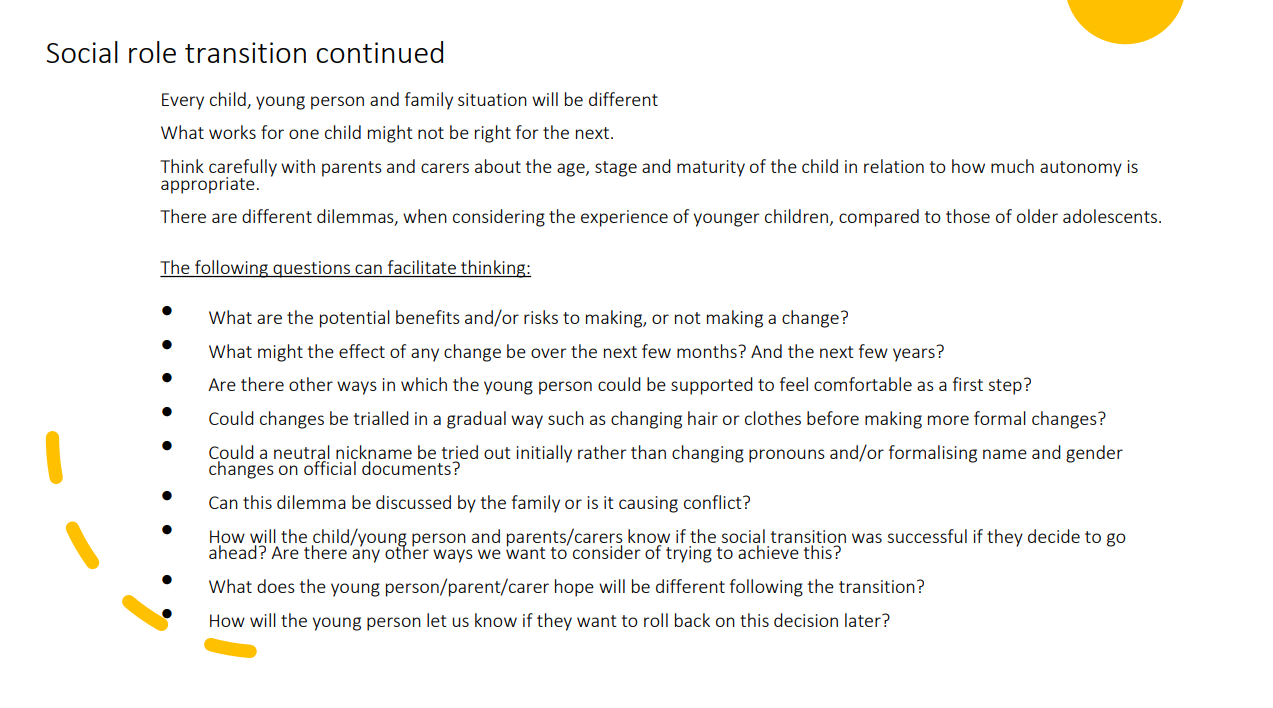
What is also striking is the way that the list of suggested “questions” to facilitate thinking are not based around focusing on following the young gender dysphoric person’s curiosity and self-directed gender exploration, and meeting them where they are. Instead they consistently prioritise attempts to minimise and restrict such exploration or self-expression. Bearing in mind this approach has nothing to do with physiological changes, it nevertheless repeatedly proposes that less gender divergent expressions are suggested as an alternative to supposedly more divergent forms of gender expression, in tiered layers, for instance, suggesting that hair or clothes be trialled before accepting a patient’s preferred name, or that a gender neutral nickname be substituted for the young person’s preference, and without using their preferred pronouns.
This repeated ratchet of pressures on gender dysphoric young people makes its value system — prioritising pushing a young patient’s gender expression to the greatest degree possible towards a cisgender norm — absolutely clear, and it is highly likely that this would be perceived by young trans people as stigmatising of their experiences, identity, and preferences, resulting in shame and harm to them. In doing this, the Gender Exploratory Model is shown to be one which primarily pathologises non-medical forms of gender expression and diversity.
Rounding out day two at the end, we have again a return to the “two perspectives” approach to support resources. These include on the one hand, two large mainstream trans charities providing support groups and services to trans and gender diverse young people: Mermaids and Gendered Intelligence.
On the other hand as the other “perspective”:
- Bayswater Support Group - Bayswater Support Group. Bayswater market a conversion therapy manual for parents by Christian conservative writer Maria Keffler, which they describe as “An essential read for parents just starting this journey with their child”.
- Genspect who’s involvement in promoting and undertaking conversion therapy has been already described above.
- Trangender Trend, who have been widely described as a hate group, and have produced guidance for schools which has been claimed to promote bullying of young trans people, and has issued schools guidance on equality issues arising from transgender students in contravention of the recommendations of the Equality and Human Rights Commission. We have also previously documented Transgender Trend's history of support for conversion therapy
Conclusion
In effect, Spiliadis, Hutchinson and Langton in their training are exercising a Teach The Controversy approach to training practitioners, where they guard against accusations of bias by presenting extremely anti-trans approaches as on an equal footing with mainstream expertise and non-medical support groups, including directing trainees towards conversion therapy resources and lobby groups.
Their therapeutic model recommends a non-patient-centred value system prioritising delaying even non-medical forms of gender expression where possible. Trans Safety Network are extremely concerned about the implications of this training continuing to be commissioned by the NHS. We are especially concerned by the fact that a professional involved in training promoting conversion therapy organisations has been hired by the Cass Review. We request that the Cass Review undertake an urgent review of their hiring practices and ensure that staff with links to conversion therapy advocacy are ruled out.
We also have grave concerns about the fact that these practitioners appear to be tightly integrated with the GIDS service, which is currently being abolished for its failures to provide adequate healthcare to trans and gender diverse youth.